













 33 / 85
33 / 85

[
] 33
suffered injuries from impact and experienced some degree of post-
traumatic stress disorder. There was also an influx of diarrhoea cases
suffered by the IDPs from nearby camps. Before adequate water and
sanitation facilities were provided at the IDP camps, an outbreak
involving more than 750 cases of acute watery diarrhoea occurred in
the unplanned, poorly equipped camp of 1,800 persons.
Despite the modest infrastructure MR operated in, the field hospi-
tal was well set up with an ambulatory consultation area, an operation
theatre and a fully stocked pharmacy. A systematic registration and
triage system was kept to record patients’ data. It ended up becom-
ing the referral hospital for WHO and the Pakistani Army, bringing
in patients who had been evacuated from the surrounding mountain
villages. In many of these referral cases, doctors were greeted with
cultural revelations on the affected community’s traditional injury
management practices. In her report,
The Lure of Pakistan: A
Humanitarian Relief Experience in Muzaffarabad
, Mercy Relief’s team
leader Dr Fatimah Lateef documented the ingenious way these
patients coped with their injuries.
3
The Kashmiris typically “covered
their wounds with turmeric powder, a spice believed to have anti-
septic properties. Some also used locks of their own cut hairs to pad
their fractured limbs, before bandaging with scarves or towels.” For
such occurrences where difficulties of immediate access to health
facilities and delayed presentation of acute injuries occurred, the risk
of wound infection and tetanus cannot be overly emphasized.
It was repeatedly documented in WHO’s
Weekly
Morbidity and Mortality Report
during the emergency
period that illnesses and deaths from tetanus had
occured due to contaminated wounds, partly due to the
low vaccination coverage among the affected popula-
tion.
4
As supplies of vaccines were limited due to
logistical constraints during the time of MR’s operations
there, MR only managed to administer the first of three
doses needed for the treatment of tetanus. Under-
treatment of tetanus had contributed to the controversies
surrounding the efficacy of vaccination efforts during
the acute emergency period. Fortunately, PIMA dili-
gently continued administering the remaining doses to
the patients. The medical personnel also had to shoul-
der the task of educating affected communities on the
functions and benefits of vaccination.
In the management of severely injured patients,
medical personnel struggled with decisions to evacuate
or isolate infected victims as this effort risked further
trauma to the victims and their dependents. In cases
where mothers were infected with tetanus and needed to
be quarantined, it proved to be a problematic arrange-
ment for the patients and their children, who required
their mothers’ continual presence and attention.
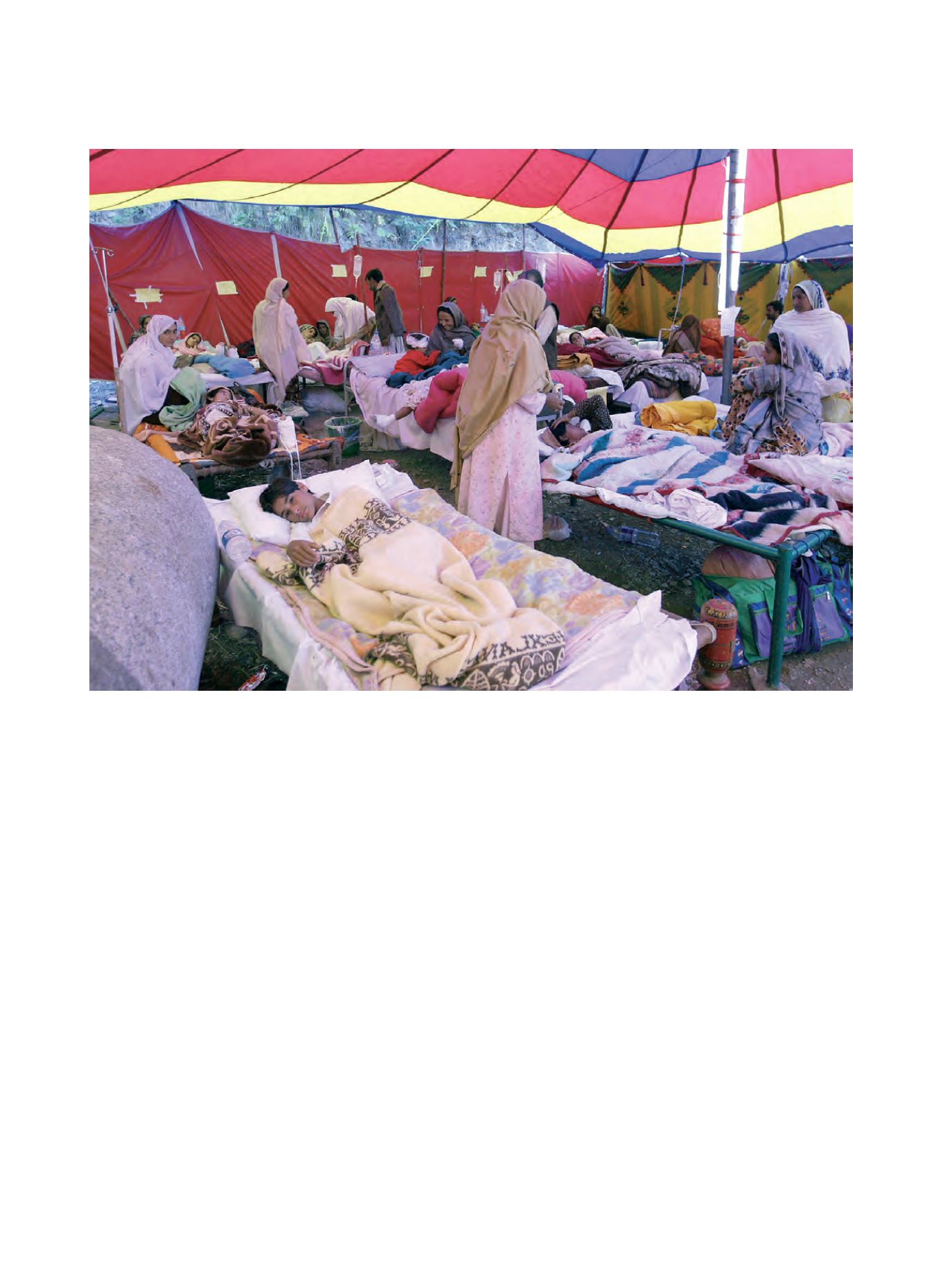
The field hospital in Muzaffarabad was overcrowded with patients and visitors, which meant medical personnel had to be vigilant in identifying and isolating
communicable disease cases to prevent any spread within the ward
Image: Terence Teo/ Mercy Relief