













 71 / 85
71 / 85

[
] 71
type 5 antibodies, had more HIV infections. A second phase-2 proof-
of-concept trial of a T-cell vaccine candidate, the Phambili study in
South Africa, was interrupted as a result of the findings of the Step
Study. The failure of the T-cell vaccines has led to a re-examination
of the HIV vaccine field, and the need to broaden research directed
at answering fundamental questions in HIV vaccine discovery through
laboratory, non-human primate, and clinical research was recognized.
The world’s leading scientists have stopped talking about vaccine
targets, instead favouring terms such as ‘incremental advances’. The
only timeframe mentioned with any confidence is 2031 – the end
point for a United Nations Aids research programme, when a vaccine
‘could be available’. But that does not mean that the quest for a
vaccine, and the funding it requires, should be diverted in any way.
The development of a polio vaccine was decades in the making. In
the 1930s claims of imminent success began to circulate, but polio
continued to cripple thousands of children every year in industrial-
ized countries. However, soon after the introduction of effective
vaccines – OPV – in the late 1950s and early 1960s, it was practi-
cally eliminated as a public health problem in the western world.
Microbicidal gels could be the key to HIV control, but they will
never have the blanket disease eradication power of a vaccine. A
medication that relies on repeat applications by an individual remains
open to considerable human error. The vaccine can generate herd
immunity to the point where, with a single jab, whole populations
can live free of the condition. It may take another 20 years, but it
will be worth the wait; the historic success of vaccines argues that
HIV vaccine research must be continued and accelerated.
Beyond the HIV vaccine
The Lancet editorial continues: “We must increase the health-systems
strengthening element to our policy and practice. We must continue
to argue for more funding. We need to rethink our approach to eval-
uating prevention. And we must find better ways to enhance
coordination between international and national actors. The very
distinction between treatment and prevention is false. Both are inex-
tricably connected. Countries need to develop context-specific
national preventive strategies, not off-the-shelf slogans dreamt up by
donors. Prevention needs to embrace the political,
economic and social determinants of risk too. The
HIV/Aids community must be more honest about admit-
ting its failures – the absolute amount of preventive
practice and science has simply been too little. The mix
of interventions has been wrong. Leadership and
management of programmes to deliver these interven-
tions have been weak. It is fair to say that, despite greatly
increased resources, the state of the response to Aids is
currently at a vulnerable moment. Implementation of
prevention strategies has been, at best, uneven across
countries – in too many instances, almost non-existent.
There is still a risk of complacency. Even Aids activists
have badly neglected prevention advocacy.”
Twenty-five years after Aids was first reported, an
institutional, commercial, professional, and even civil
society industry now controls the global response to
Aids. Each party, in good faith, has a position to defend,
a strategy to advance, and probably someone to oppose.
It is time for new voices in Aids to ask questions, to
disrupt axes of power, and to disturb the air.
4
The
lessons learned over the past 25 years should be used to
provide the foundation on which to build comprehen-
sive, sustainable, nationally owned responses that are
vital to the ultimate control of this pandemic.
5
The question of rights of participants, access to stan-
dard of care and of possible research injury in HIV
biomedical prevention trials
6
are relevant, considering the
unfavourable results of HIV vaccine trials thus far and the
risk of becoming HIV positive. The role of ethics commit-
tees, data and safety monitoring boards and community
advisory boards in this context is therefore critical, where
the participants are usually socio-economically deprived.
The South African HIV/Aids Research and Innovation
Platform (SHARP) has recently been established by the
Department of Science and Technology and is being
managed by LIFElab. It has the objective of increasing
the number and quality of South African developed
products and services for the prevention and treatment
of HIV/Aids through increased support for basic and
applied research, development and innovation in the
areas of anti-retrovirals, microbicides, vaccines and
diagnostics.
“In recent weeks we have seen governments across the
world working together to solve the global financial
crisis,” says Stephen Matlin of the Global Forum for
Health Research. “No one country can ignore what has
been happening, and by working together, governments
know they have more chance of affecting real change. In
the same way, the global community must act together to
invest in health research and achieve global health gains.”
Similarly, the academic and biotechnology sectors glob-
ally need to partner and collaborate in seeking the elusive
holy grail of a safe and effective HIV vaccine. Further,
the recent USD100 million gift to create an institute to
jumpstart the search for an HIV vaccine in Cambridge,
USA, is a positive development in view of shrinking
endowments and broke donors, as a result of the global
economic slump.
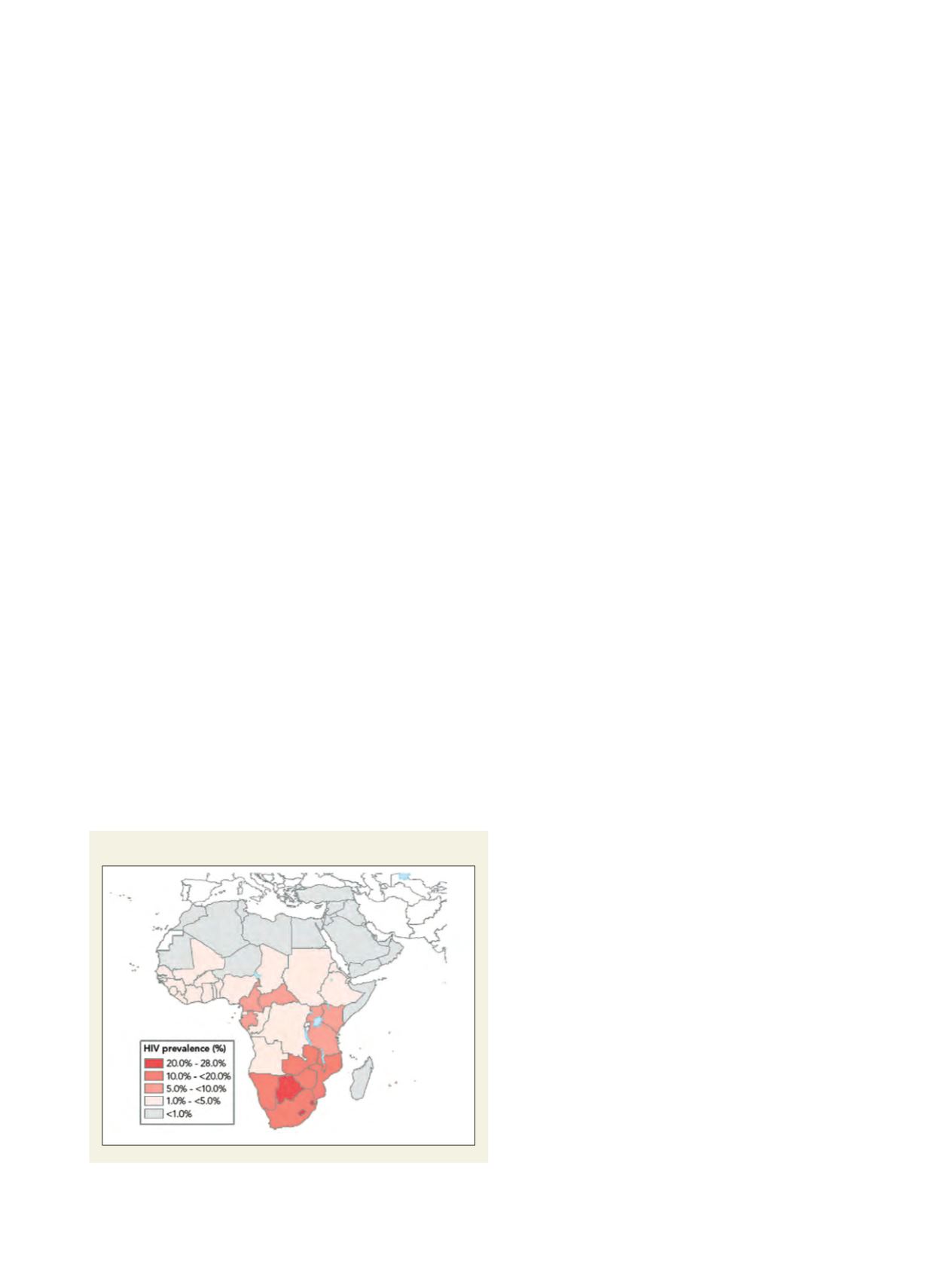
HIV prevalence (%) in adults (15-49) in Africa, 2007
Source: UNAids Report 2008